











































Theory-based Development of an Implementation Intervention to Increase HPV Vaccination in Pediatric Primary Care Practices
Washington University (Garbutt); Washington University School of Medicine (Garbutt, Dodd, Walling, Lee, Kulka, Lobb); University of Michigan (Walling)
In 2016, 10 years after the human papillomavirus (HPV) vaccine was first introduced in the United States (US), only 49.5% of eligible females and 37.5% of eligible males aged 13-17 years had completed the vaccine series. This paper describes the systematic process of applying theory to develop a pragmatic intervention to increase use of HPV vaccine as recommended in the US Centers for Disease Control and Prevention (CDC) guidelines. The study is grounded in the conviction that improving use of evidence-based practices requires behaviour change and that, in order to design effective interventions and allow purposeful improvements when interventions fail, it is necessary to understand these behaviours in context.
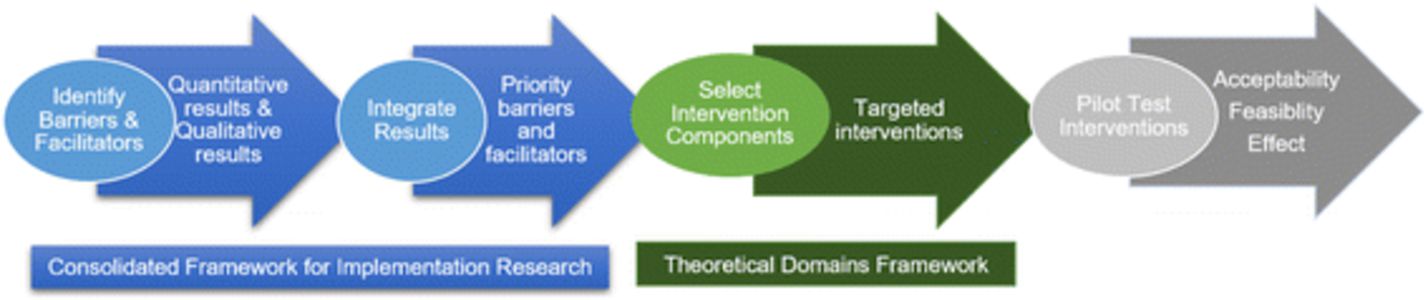
Sixteen providers (community paediatricians and paediatric nurse practitioners associated with Washington University) from 10 practices comprised the study sample. In order to identify barriers and facilitators to guideline-recommended HPV vaccine use, the researchers used the Consolidated Framework for Implementation Research (CFIR), which identifies 5 major domains of organisational context that influence successful implementation: characteristics of the implementation intervention, the inner setting (the context through which implementation will proceed), the outer setting (the context in which the organisation resides), implementer's characteristics, and the processes of implementation. The provider interview guide addressed the main CFIR constructs and included both general and specific open-ended questions. The interviews were conducted at the practices between January 27 2016 and May 24 2016.
All providers were aware of the CDC recommendations to complete the HPV vaccine series by age 13 and universally assumed responsibility for vaccine delivery. Providers typically recommended initiation and completion of the HPV vaccine series during 11- to 12-year-old well visits; however, the strength of this recommendation varied. Most providers felt that information about vaccine benefits was needed to counter the misinformation parents received from the media and other sources. To meet this perceived need, providers routinely informed parents that HPV vaccine prevents cancer; providers varied in sharing personal information about vaccinating their own children or grandchildren. All providers used the vaccine information sheets (VIS) from the CDC to provide parental education.
Commonly reported difficulties with providing HPV vaccine included taking longer to discuss HPV vaccine than other vaccines and dealing with the resistance and hesitancy of parents. Many felt they could not persuade hesitant parents to provide HPV vaccine for their child, and some preferred to delay discussion of prevention of a sexually transmitted cancer until the child was older and the parent was more accepting.
The researchers then used the Behavior Change Wheel (BCW) and the Theoretical Domains Framework (TDF) to analyse provider behaviour and identify behaviours to target for change and behavioural change strategies to include in the intervention. The TDF is a theoretical framework with 14 theoretical domains covering the main factors influencing provider's clinical behaviours and behaviour change. These domains have been linked to a simplified model of behaviour change, the COM-B model, which characterises behaviour change in terms of capability, opportunity, and motivation (COM-B). The BCW illustrates the interventions and behaviour change functions that link the TDF to the COM-B model.
From these analyses, the researchers found these distinguishing factors between higher and lower coverage related to provider characteristics: their lack of buy-in to vaccination by age 13, their lack of confidence to address parental hesitancy, and poor communication skills to promote timely HPV vaccine use. Also, coverage was higher in practices with coordination between the provider and staff. They concluded that the provider was the one whose behaviour needed to change to increase vaccine coverage, and they identified 3 targeted behaviours: (i) recommend getting the HPV vaccine in the same way and at the same time as other adolescent vaccines; (ii) answer parents' questions about the vaccine with confidence; and (iii) work with staff and providers to develop a vaccine delivery system using all possible resources.
To this end, the intervention targeted improving providers' capability (knowledge, communication skills) and motivation (action planning, belief about consequences, social influences) regarding implementing guideline recommendations and increasing their opportunity to do so (vaccine delivery system). Behaviour change strategies included providing information and communication skill training with graded tasks and modeling, feedback of coverage rates, goal setting, and social support. These strategies were combined in an implementation intervention to be delivered using practice facilitation, educational outreach visits, and cyclical small tests of change.
Finally, educational materials for the parent were developed, as those currently available to provide information about HPV vaccine were judged to be inadequate. Specifically, parent advisors felt the CDC brochures contained too much information, and providers wanted a generic brochure that could be used for girls and boys. So, the researchers develop posters and a brochure, tested their acceptability with a sample of 21 parents recruited from study practices, and revised them to include their suggestions for improvement and address their concerns.
The researchers conclude: "Our hope is that this multi-component intervention designed to address multiple barriers will have a greater and more sustainable effect on HPV vaccine use than prior interventions focused on one or two barriers."
Implementation Science (2018) 13:45. https://doi.org/10.1186/s13012-018-0729-6
- Log in to post comments