











































Evaluation of the Functionality and Effectiveness of the CORE Group Polio Project's Community-Based Acute Flaccid Paralysis Surveillance System in South Sudan
CGPP/South Sudan (Kisanga, Abiuda); HIGH PSL 9114 LTD. (Walyaula, Samson); CGPP (Losey)
"Community-based surveillance represents a powerful tool for disease control that merits broader application..."
Although the last indigenous wild poliovirus (WPV) case was reported in 2001, South Sudan experienced large imported WPV outbreaks in 2004, 2005, 2008, and 2009, affecting 9 of the 10 states. In October 2015, in response to the destruction of the existing surveillance system, the CORE Group Polio Project (CGPP) designed and implemented a community-based surveillance (CBS) system in 34 counties of the most war-affected states of Unity State, Jonglei, and Upper Nile. This evaluation assesses the functionality and effectiveness of the community-based acute flaccid paralysis (AFP) surveillance system designed and implemented by CGPP in conflict-affected and inaccessible areas of South Sudan between October 2015 and September 2017. It is part of a series of articles detailing the work of the United States Agency for International Development (USAID)-funded CGPP (accessible through Related Summaries, below).
The CBS system in South Sudan is based on the assumption that the relatively rare event of acute onset paralysis in a child will elicit some form of health-seeking behaviour (e.g., a mother taking a child to a traditional healer), which will become known throughout the community and, in particular, to various influential individuals. Whereas international non-governmental organisation (NGO) and United Nations staff would not be able to travel to insecure areas of the war-torn country, the idea is that national NGOs could hire and train local staff already in these areas to train and supervise the community-based informants. (The CGPP developed standard operating procedures that include a supportive supervision checklist and a field activity log book.)
The CGPP CBS system has 34 county supervisors who oversee the system at the county level. A total of 230 payam (subcounty) assistants were recruited and deployed at the payam level to supervise the activities of 3,228 community key informants, whose task is to detect and report any suspected AFP cases in their villages. The informants are mostly illiterate but respected in the community. They include traditional healers, teachers, church leaders, chiefs, traditional birth attendees, women leaders, and youth leaders. The CBS system does not expect the informants to actively work as surveillance personnel, and they are not paid.
The evaluation methodology consisted of a desk review of key CGPP and World Health Organization (WHO) surveillance documents, reports at the national level, and interviews with key informants at the county level. In addition, interviews and focus group discussions were conducted with relevant partners and stakeholders. Quantitative data were obtained from routine reports of the CGPP CBS system and the WHO line-list for 2016 and 2017.
To assess whether the CBS system is effective, the evaluation looked into 3 aspects of surveillance: (i) Did the number of AFP cases reported increase with time (i.e., did the sensitivity increase)? (ii) Was the reporting of AFP cases timely? (iii) Was the follow-up investigation of reported cases of AFP cases timely? Data is shared, along with quotations from research participants that provide additional insights.
The evaluation found that South Sudan's CGPP CBS system, implemented in inaccessible, insecure, and hard-to-reach areas of the country, is functioning effectively, with a well developed network of 2,366 male and 1,126 female community informants, payam assistants, and county supervisors. Within 24 months after the initiation of the CBS system, 100% of the staff were in place, the staff and volunteers were able to clearly define their roles and responsibilities, trainings were being offered, community meetings to sensitise the communities on AFP were being held, clear reporting lines were identified, and active supervision by both the county supervisors and payam assistants was underway. The CBS system monitoring tools were being used to document surveillance activities.
Data shared include:
- There was an increase from 0.0% to 56.4% of cases reported through the CBS system between January 2016 and June 2017, and 80.0% of the cases reported within WHO standards of 24–48 hours were through the CBS system, whereas 20.0% were through the facility-based system.
- The CBS system also recorded an increase from 36.0% in 2014 to 92.0% in December 2016 for the number of counties that were reporting AFP.
- Between January 1 2017 and June 30 2017, nearly three-quarters of the total AFP cases reported from the geographic areas where the CGPP was operating were obtained from the CBS system, compared with only one-quarter from the facility-based system.
- More than three-quarters of the AFP cases reported through the community-based system between January 1 2017 and June 30 2017 were reported within the recommended reporting timeframe by community key informants.
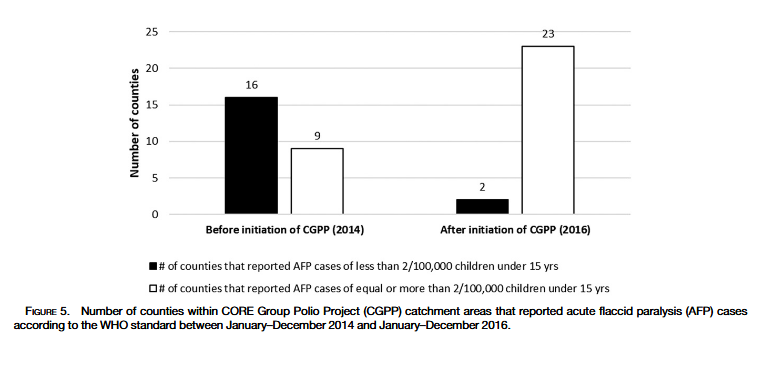
- Analysis of data from 25 counties in the conflict-affected states of Upper Nile, Jonglei, and Kapoeta East county before the initiation of the CBS from January to December 2014 and other data for the period January-December 2016 after the initiation of the CBS system in these CGPP catchment areas indicated that there was substantial increase in the number of counties that reported AFP cases in 2016 compared with 2014 before the introduction of the CBS system.
Thus, the evaluation found that, despite challenging field conditions produced by insecurity, lack of roads, and intermittent flooding, the CGPP CBS system in South Sudan expands the effectiveness of surveillance that was previously only available through a passive facility-based system in which children with paralysis were brought to a health facility for treatment.
Field interviews indicated that factors that contributed to the effective functioning of the CBS system were:
- The presence of a network of community key informants in every village;
- The presence of supervisory staff who can investigate AFP cases promptly;
- Strong capacity building through training, close supervision, awareness creation, and involvement of the local community;
- Strong coordination;
- Partnerships - e.g., the CGPP established partnerships with other key players - local and international - to reach greater numbers of people, particularly displaced populations.
As reported here, the CGPP is now positioned to use the community engagement required for the CBS system for promotion of routine immunisation, guinea worm eradication, and control of other communicable diseases such as tuberculosis, kala-azar, measles, and neonatal tetanus. Such systems could also identify cases of Ebola and pandemic influenza.
In conclusion, a CBS system is "a valuable complement to facility-based surveillance in insecure environments or where the population has limited access to facilities."
American Journal of Tropical Medicine and Hygiene, 101(Suppl 4), 2019, pp. 91-99. https://doi.org/10.4269/ajtmh.19-0120.
- Log in to post comments