











































Improving Immunisation Coverage in Ethiopia: A Formative Evaluation in Pastoral Communities
Center for National Health Development in Ethiopia, or CNHDE (H. D. Teklehaimanot, G/Michael, A. Teklehaimanot); Oromia Regional Health Bureau, or ORHB (Tolera)
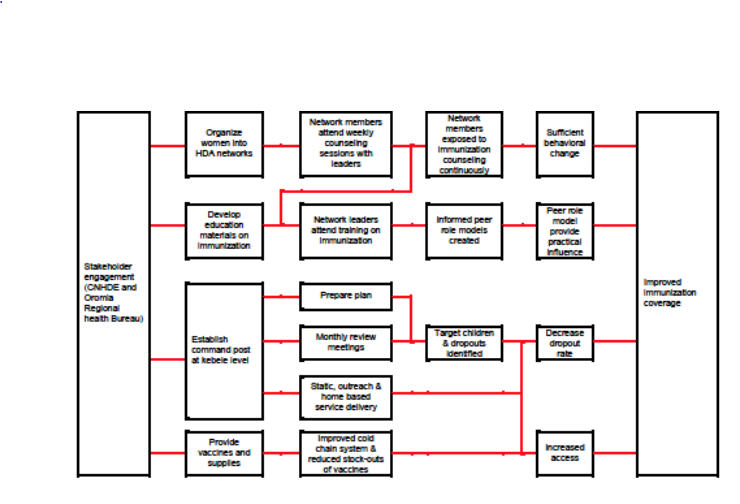
"Did peer role models influence community members to adopt immunization? Has immunization coverage improved?"
In Ethiopia, approximately 15 million people practice pastoralism. Access to and utilisation of immunisation services in pastoral areas are lower than those among sedentarised communities. The key factor contributing to poor service demand is lack of awareness and understanding of health matters, risk factors, and modern health services stemming from inadequate exposure to channels of behavioural communication services (due to constant mobility and low socio-economic status), low status of women, harmful traditional practices, and low educational attainment. With the aim of empowering communities and addressing demand-side barriers in the health system, the Ethiopian government introduced a community mobilisation platform called Health Development Army (HDA) in 2011/2012. This International Initiative for Impact Evaluation (3ie) report shares details on a project implemented in Borena zone in the Oromia Regional State of Ethiopia with the objectives of organising pastoral women into networks of HDA and evaluating the implementation process and its contribution to improvement of immunisation.
As part of the intervention, health extension workers (HEWs) trained women from the community to become HDA members and drive health-related behaviour change within their communities. Unlike the providers of formal health services who remain static in terms of location, the HDA members remained with their pastoral communities and were responsible for health-service-related engagements.
Selected women community members were systematically trained in immunisation, as well as other services that are part of the health extension programme package and in accordance with the government policy. The HDA network consisted of development teams and 1-5 networks (5 members and 1 leader, who is a model woman practicing healthy behaviours, which enables her to influence fellow network members, to counter negative opinions, and to respond to their questions and concerns). Development teams were organised in 20-30 households clustered in 1-5 networks (organised in a group of 6 households) living in the same neighbourhood. The network leader reported to development team leaders, who were in turn supervised by HEWs. In addition, the intervention engaged traditional leaders (locally known as abba ollas), who were consulted during the formation of networks, as well as for the election of the network and development group leaders. Due to the frequent location change within the village and to ensure the sustainability of network organisation even after families migrate, pastoral women were organised into the HDAs based on their abba olla.
The HDA model is based on diffusion theory, which stipulates that interpersonal contact through social systems and networks provides information and influences opinion and judgment among community members. Innovators and early adopters who embrace change opportunities after training - these are the "leaders" in the 1-5 networks - serve as intermediary change agents, while opinion and community leaders exert influence on community member behaviour via their personal contacts. The following underlying assumptions support this theory:
- Peer-to-peer counselling and experience sharing on immunisation, through frequent and regular meetings, can produce sufficient behavioural change leading to improved immunisation.
- The network meetings continue when the community moves away from their kebeles, ensuring continuity in behavioural communication activities.
- The intended beneficiaries (i.e., pastoral women) are correctly identified, and women with children are included in the network.
To cite one example of HDA activities: The 1-5 network leaders educate, influence, and persuade 5 fellow network members by organising weekly regular meetings, during which they: provide education and counseling to network members; offer peer-to-peer counseling and share individual experiences; create and update community vital events registers to list all infants and record their vaccination dates; provide practical evidence such as individual success stories and benefits of immunisation; evaluate individual and group performance; motivate mothers when a child falls behind in the immunisation schedule; and develop individual and group plans for the following week.
Additional activities in the implementation of the intervention include provision of supplies and equipment necessary for static and outreach services to improve the supply-side aspect, with special focus on cold chain management. HEWs ensure that the health post is open for the public daily and provide health services, including immunisation, as appropriate at the health post, outreach, and/or household level.
This study incorporated both quantitative and qualitative methods. The qualitative component employed 8 community focus group discussions (representing different stakeholders) and 45 key informant interviews. In addition, all households at baseline (December 2016) and households with under-5 children at endline (June 2017) were surveyed using structured questionnaires upon verbal consent.
The percentage of fully vaccinated 1-year-old children in the communities increased from 26.6% at baseline to 52.4% at endline. The immunisation coverage among 1-year-old children of mothers who participated all or most of the HDA network meetings was the highest (69.4%) compared to the coverage among children of mothers who participated in some of the meetings (51.5%) and few or none of the meetings (39.6%).
The intervention was found to be highly acceptable by health staff, the intended beneficiaries, and HEWs. Ninety-seven percent of 968 women during endline reported they had heard about the HDA, and 96.3% of these women were members of the HDA network. However, only 9.3% of the HDA members attended all scheduled meetings, and only 14.5% attended most of the scheduled meetings. The most frequently stated reason for low attendance was the increased mobility of the community members due to severe drought conditions during the intervention period.
Elements found to be supportive of the successful implementation of the intervention include: engagement and participation of different stakeholders at different levels of the project; equipping of network leaders with adequate knowledge and skills; participation of traditional leaders in support and supervision of networks; timely identification of challenges and consideration of inputs from stakeholders into the intervention design; ownership of the intervention by the public sector (implementing agency of the project), facilitating linkage with the health system; the sense of community ownership and empowerment created; the parallel strengthening of outreach services improving the supply-side barriers; the timeliness of the project responding to the government and community needs; and the fact that the networks served as a platform to address other social issues.
Lessons learned include:
- In communities with strong traditional leadership systems, it is critical to first engage and convince the traditional leaders who, if convinced, would ensure successful implementation of community engagement interventions. This approach creates community-level consensus (that includes husbands), ensuring women's right to participate in community engagement activities.
- The expected roles and responsibilities of community members in community engagement intervention should be determined based on their educational level.
- When the community has other major problems and competing priorities, it is difficult to engage the community and introduce new health interventions. The communities are not interested in other issues at times of severe drought, for example, when they are busy ensuring that their cattle have enough water to drink.
- What may not be a sensitive question in some communities could be sensitive in other communities. For instance, in the pastoral areas, asking question regarding the number of cattle a person owns is sensitive.
- The HDA model requires temporary reconstitution and regrouping of members when network members partially migrate. To ensure independent reorganisation by the members themselves, the team suggests strategies such as entrusting members with identifying women who migrated with them and initiating the creation of temporary networks of these women.
Given the findings of feasibility, acceptability, and potential benefits in improving immunisation rates, the authors recommend a full impact evaluation to determine the intervention's impact on immunisation coverage and health status of children, cost-effectiveness, and sustainability.
3ie website, July 30 2019.
- Log in to post comments