











































Obstetrician-Gynecologists' Strategies to Address Vaccine Refusal Among Pregnant Women
University of Colorado Anschutz Medical Campus, and Children's Hospital Colorado, Aurora, Colorado; the American College of Obstetricians and Gynecologists; Centers for Disease Control and Prevention, or CDC; Denver Health
Conducted among a national sample of obstetrician-gynaecologists (ob-gyns) in the United States (US), where uptake of vaccines in pregnancy is suboptimal, this study sought to describe practices and attitudes regarding vaccination of pregnant women. Particular areas of exploration include: barriers to use of standing orders for vaccination; perceived frequency of vaccine refusal among pregnant patients and reasons for refusal; strategies used when encountering vaccine refusal and their perceived effectiveness; and barriers to discussing the risks and benefits of vaccines with pregnant women.
The study was carried out between March 2016 and June 2016 by the Vaccine Policy Collaborative Initiative, which is a programme designed and implemented collaboratively with the Centers for Disease Control and Prevention (CDC). Physicians (n = 331) were surveyed through the internet or, if they preferred, by mail. Among the findings:
- Almost all respondents reported strongly recommending both influenza (97%) and tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) (95%) vaccines to pregnant women.
- Almost all ob-gyns strongly agreed that it was safe to give both Tdap and influenza vaccines to pregnant women. Ob-gyns' attitudes were in concordance with current recommendations.
- Regarding time spent discussing vaccines with a pregnant woman in need of vaccines who had no concerns, 12% of respondents reported "no time or someone else discusses", 69% reported 1-2 minutes, 17% reported 3-5 minutes, and 3% reported 6 or more minutes. For women with substantial vaccine concerns, 1% reported "no time or someone else discusses", 7% reported 1-2 minutes, 54% reported 3-5 minutes, and 38% reported 6 or more minutes.
- Overall, 62% of ob-gyns reported that 10% or more of their pregnant population refuses influenza vaccine compared with 32% reporting this for Tdap. Factors most commonly reported by respondents as contributing "a lot" to refusal included belief that influenza vaccine makes them sick, belief they are unlikely to get a vaccine-preventable disease, general worries about vaccines, the desire to maintain a natural pregnancy, and concern their child could develop autism as a result of receiving a vaccination during pregnancy. (According to the researchers, this latter finding underscores the profound influence of safety information on vaccines, even if erroneous, on the decisions of pregnant women.)
- Almost all ob-gyns strongly agreed they were comfortable discussing influenza and Tdap vaccines with pregnant patients (98% and 96%, respectively). Fewer, however, agreed that they were comfortable addressing questions or concerns about the infant series of vaccines (18% strongly agree, 31% somewhat agree, 34% somewhat disagree, 16% strongly disagree).
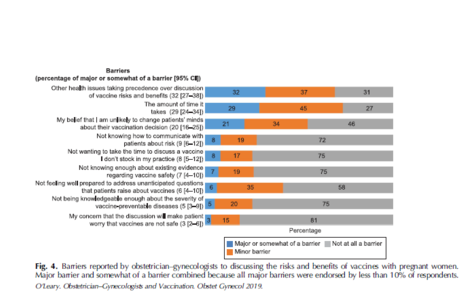
- The most common barriers to discussing the risks and benefits of vaccines with pregnant women were other health issues taking precedence and the amount of time it takes. The only other barrier endorsed as "major" or "somewhat" by more than 10% of respondents was "my belief that I am unlikely to change patients' minds about their vaccination decision".
- Strategies ob-gyns reported as always or often used by more than half of healthcare providers when encountering a pregnant woman refusing a vaccine included: expressing confidence that it is safe to receive vaccines in pregnancy (96%), explaining that not getting the vaccine puts the fetus or newborn at risk (90%) or the pregnant woman's health at risk (84%), discussing outbreaks of vaccine-preventable diseases (72%), informing the patient that not getting the vaccine is against the healthcare provider's recommendation (64%), and stating that they personally would get the vaccine or give it to a family member if pregnant (53%). In general, most of these strategies were perceived by a majority of physicians as "somewhat effective"; the only strategy that stood out as being perceived as "very effective" by a substantial proportion of physicians (40%) was explaining that not getting the vaccine puts the fetus or newborn at risk.
Although the focus of this article is on vaccine refusal, it also reports on use of standing orders, which is an approach sending the message to both healthcare professionals and patients that vaccination is the default option. In addition to increasing vaccination coverage and efficiency, standing orders - an example of a social norm - may overcome attitudinal barriers. Science in other areas shows that "nudges" can be effective at overcoming attitudinal resistance to a desired behaviour. Barriers to use of standing orders could be surmounted, according to the researchers - for example, patients who prefer to speak with the healthcare provider before vaccination may still do so.
In conclusion, the study found few attitudinal barriers regarding vaccination among ob-gyns themselves. However, the majority of US ob-gyns perceive that vaccine refusal among pregnant women is common, particularly for influenza vaccine. Studies support the claim that vaccine refusal among pregnant women may be more common than parental refusal of childhood vaccines. The ob-gyns report using a number of different strategies for addressing vaccine refusal, yet only one - explaining that not getting the vaccine puts the fetus or newborn at risk - was perceived as very effective. "Future work should focus on testing evidence-based strategies for addressing vaccine refusal in the obstetric setting and understanding how the unique concerns of pregnant women influence the effectiveness of such strategies."
Obstetrics & Gynecology: January 2019, Volume 133, Issue 1, p 40-47 doi: 10.1097/AOG.0000000000003005
- Log in to post comments