











































One Size Doesn't Fit All: Methodological Reflections in Conducting Community-based Behavioural Science Research to Tailor COVID-19 Vaccination Initiatives for Public Health Priority Populations
Ottawa Hospital Research Institute (Fontaine, Langmuir); University of Ottawa (Fontaine); Citizen Partner (Smith) - plus see below for full authors' affiliations
"There is a need to conduct community-based, behavioural science research with marginalized populations to identify community-specific and responsive solutions."
Promoting the uptake of vaccination for infectious diseases such as COVID-19 remains a global challenge, necessitating collaborative efforts between public health units (PHUs) and communities. Applied behavioural science can support PHUs' response by providing insights into human behaviour and informing tailored strategies to enhance vaccination uptake. Community engagement can help broaden the reach of behavioural science research by involving a more diverse range of populations and ensuring that strategies better represent the needs of specific communities. This paper presents the methodology developed for community engagement with ethnically and socioeconomically diverse populations in Ontario, Canada, to conduct behavioural science research to guide PHUs in their strategies to promote COVID-19 vaccination uptake. It shares lessons learned in applying the methodology, covering key considerations for fostering effective research partnerships with communities.
The research team included behavioural scientists, health services researchers, and a citizen partner with extensive experience in COVID-19 citizen engagement. They collaborated with PHUs and local communities in Ontario, Canada to identify priority groups for COVID-19 vaccination, understand factors influencing vaccine uptake, and co-design strategies tailored to each community to promote vaccination. Community engagement was conducted across three large urban regions with individuals from Eastern European communities, African, Black, and Caribbean communities and low socioeconomic neighbourhoods.
The seven-step community engagement methodology for conducting community-based behavioural science research was developed based on integrated knowledge translation (iKT) and community-based participatory research (CBPR) principles. It includes:
- Aligning goals with system-level partners - This step occurred during the second year of the COVID-19 pandemic, when the first few waves had passed, and vaccines were readily available. On a societal level, some of the trust that characterised the early stages of the pandemic was eroding or lost.
- Engaging with PHUs to understand priorities - Working with PHUs, the research team employed a prioritisation matrix to determine the focus on specific vaccination doses and communities.
- Understanding community strengths (sociocultural, health-seeking) and vaccination behavioural dynamics - The research team first held meetings and engaged with community leaders in Ottawa, Peel Region, and Toronto. In parallel, they conducted a detailed environmental scan to identify how the three PHUs promoted COVID-19 vaccination amongst key populations, to classify existing strategies/resources used by these PHUs, and to identify the barriers and enablers to vaccination that these strategies are designed to address.
- Building relationships with each community - The main principles of the community engagement framework were introduced during initial discussions with community leaders. This framework emphasised mutual respect, shared decision-making, and measures to promote equitable partnerships, reduce power imbalances, and enhance the validity and relevance of research conducted.
- Establishing partnerships (community advisory groups, or CABs) - This process involved working with PHUs to identify community leaders or organisations who would then select members to form CAGs for each city. Each CAG, comprising 5 to 10 members per PHU, collaborated with the team on key research activities, such as recruiting individuals for qualitative interviews.
- Involving community members in the research process - With support from the CAGs, the research team conducted theory-informed interviews guided by the Theoretical Domains Framework (TDF) and explored barriers and enablers to COVID-19 vaccination along 14 domains (e.g., environmental context and resources; social influences; emotion; behavioural regulation). They conducted 14 interviews with people who were not vaccinated, 3 with people who had the first dose, 36 with people who had the second dose, and 15 people who had 3 or more doses.
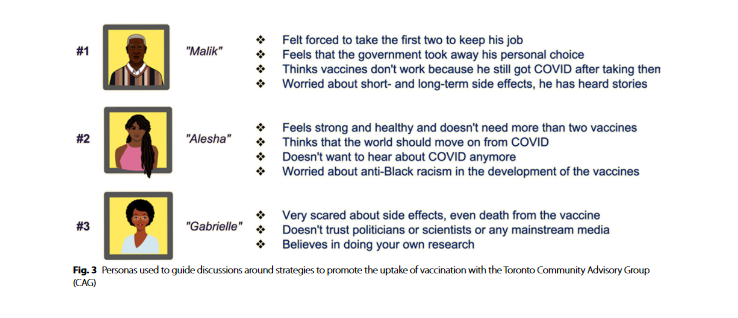
- Feeding back and interpreting research findings - The team, with CAGs, developed "personas", who represented fictitious individuals in each community, as a way of presenting the themes and perspectives derived from the qualitative interviews. In-depth feedback sessions enabled members of each CAG to validate recommendations emerging from their community before they were shared with PHUs. The research team held a final meeting with each CAG to reflect on collective progress, areas of learning and mutual growth, and wasy in which their input directly influenced public health recommendations. Members of each CAG also received the findings of an independent evaluation of the engagement process to demonstrate the value of the study. Recommendations were then shared through policy briefs with key stakeholders from each PHU, and meetings were held to discuss recommendations. Sample recommendation: Identify examples from within communities where people have changed their minds about the vaccine to amplify (e.g., on video screens displayed while people are waiting at wellness clinics), especially featuring stories from local community leaders, community ambassadors, and relatable "regular people".
Lessons learned include the importance of: cultivating cultural sensitivity and awareness of sociopolitical context in tailoring community engagement, being agile to address the diverse and evolving priorities of PHUs, and building trust to achieve effective community engagement. For instance, in Toronto, where prioritised populations were African, Black, and Caribbean communities, discussions reflected the community leaders' expertise in their communities and were focused on intersectional issues and structures of power within society. They helped the research understand the factors that influenced their community's behaviours and what could potentially be done to repair relationships, and they provided messaging that resonated with their communities. There were open and honest conversations about how unethical research and systemic racism continues to have profound repercussions on African, Black, and Caribbean communities' relationships with the healthcare system, the government, and the scientific community. In such a context, the trust-building process in this study was crucial. The team identified 5 key trust-building mechanisms based on their experience: (i) getting acquainted; (ii) ensuring cultural and linguistic competence of the research team; (iii) working out differences and resolving conflicts; (iv) acknowledging the validity of mistrust and damaged relationships based on past experiences; and (v) addressing ethical considerations and ensuring reciprocity.
Reflecting on the experience, the research team notes that, "When community engagement results in a positive, rewarding experience, community members are more willing and capable of advocating for inclusion in research that concerns them, as well as communicating to researchers which factors contribute to effective participation in the research process. At various points throughout the study, community members shared positive feedback on their engagement experiences. Many community partners from all three geographical regions elected to be notified of future opportunities to collaborate with research teams."
In conclusion: "As citizen engagement in health research becomes more common, best practices need to reflect the diversity of communities and how the engagement approach must not be conceived as 'one size fits all.'...[I]ncreased public interest in science and public health since the outbreak of the COVID-19 pandemic, including both positive and negative perceptions, should be responded to by researchers with active engagement efforts. As researchers, we have an opportunity to highlight the value of community engagement and bring community members together to tackle complex public health issues such as climate change, environmental destruction and food insecurity. Combining community engagement and behavioural science approaches can result in public health policies and recommendations that are truly relevant and meaningful to diverse communities."
Full list of authors, with institutional affiliations: Guillaume Fontaine, Ottawa Hospital Research Institute and the University of Ottawa; Maureen Smith, Citizen Partner; Tori Langmuir, Ottawa Hospital Research Institute; Karim Mekki, Ottawa Public Health; Hanan Ghazal, Ottawa Public Health; Elizabeth Estey Noad, Peel Public Health; Judy Buchan, Peel Public Health; Vinita Dubey, Toronto Public Health; Andrea M. Patey, Ottawa Hospital Research Institute, School of Epidemiology and Public Health, and Queen's University; Nicola McCleary; Ottawa Hospital Research Institute; Emily Gibson, Ottawa Hospital Research Institute; Mackenzie Wilson, Ottawa Hospital Research Institute; Amjad Alghamyan, University of Ottawa; Kateryna Zmytrovych, Citizen Partner; Kimberly Thompson, The Hospital for Sick Children (SickKids); Jacob Crawshaw, McMaster University; Jeremy M. Grimshaw, Ottawa Hospital Research Institute, University of Ottawa, and School of Epidemiology and Public Health; Trevor Arnason, Ottawa Public Health; Jamie Brehaut, Ottawa Hospital Research Institute and School of Epidemiology and Public Health; Susan Michie, University College London; Melissa Brouwers, Ottawa Hospital Research Institute and School of Epidemiology and Public Health; and Justin Presseau, Ottawa Hospital Research Institute, School of Epidemiology and Public Health, and University of Ottawa
BMC Public Health 2024; 24: 784. doi: 10.1186/s12889-024-18270-x.
- Log in to post comments