











































Trial of a Novel Intervention to Improve Multiple Food Hygiene Behaviors in Nepal
London School of Hygiene and Tropical Medicine (Gautam, Schmidt, Cairncross, Curtis); Freelance Consultant (Cavill)
"This study suggests that it is possible to change entrenched food hygiene habits, even in environmentally challenging conditions such as pertain in rural Nepal."
This paper reports on a trial of an intervention to improve 5 food hygiene behaviours among mothers of young children in Kavre District in the highland area of rural Nepal. The intervention was based on motivating mothers rather than educating them using a creative approach and behaviour change science. The purpose of the initiative was to explore whether a systematically designed, scalable intervention underpinned by an explicit theory of change could improve multiple food hygiene behaviours in the challenging context of rural Nepal, where diarrhoea is the second most important cause of death in under-fives, and 41% of children are stunted.
The campaign's theory of change was that mothers would identify with a central "ideal mother" character, who practiced safe hygiene so as to be respected in the community (Status motive). Nurture, Disgust, and Affiliation were further levers of change, and the goal was to disrupt daily food preparation habits that were held in place by tradition, routine, and the social and physical settings of kitchens. Based on formative research and a creative process using the Behavior-Centered Design (BCD) approach, the intervention package was designed and delivered over a period of 3 months (May-August 2013). Specifically, underpinned by the Evo-Eco theory of change, BCD has 5 steps, which are described in detail in the paper (and in the video, below); in brief:
- A: Assess - the collection and analysis of published and local knowledge concerning food hygiene behaviour to define target behaviours, the parameters of the intervention, and the questions to be answered in the formative research.
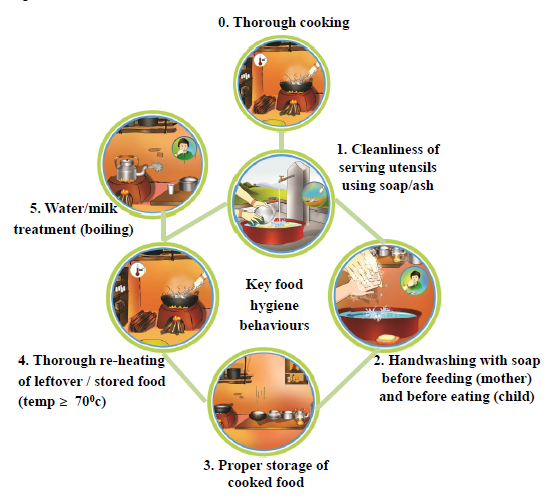
- B: Build - a Hazard Analysis and Critical Control Points assessment that led to the identification of 5 behaviours to target: cleanliness of serving utensils, handwashing with soap before feeding, proper storage of cooked food, and thorough reheating and water treatment.
- C: Create - the assembly of a local creative team with expertise in marketing, design, innovation, programme development, and behaviour change.
- D: Deliver - delivery through 6 events (local rallies, games, rewards, storytelling, drama, competitions linking with emotional drivers of behaviour, and "kitchen makeovers" to disrupt behaviour settings), followed by 6 household visits from 15 trained Food Hygiene Motivators (FHMs). FHMs with a similar profile to Nepal's ubiquitous Female Community Health Volunteers (FCHVs) were recruited locally and trained to implement the campaign. Nurture-based activities included a game about the child's life, an exchange of letters, and a family drama. Affiliation-based activities included a folk song, a puzzle game, peer review, and cookery demonstration. Disgust-based activities included a Glo Germ demonstration and a hot potato game. Status-based activities included a public pledging, public display of photos of ideal mothers, and declarations of safe food zones. The social and physical settings of kitchens were disrupted by holding makeover parties where the kitchen was redecorated using coloured bunting and danglers placed at eye level and when neighbours agreed to practice new hygiene rituals. Villages were then declared "safe food hygiene zone," with volunteer mothers becoming food hygiene monitors.
- E: Evaluate - the conducting of a study between October 2012 and December 2013, described below.
The effect of the package on behaviour was evaluated via a cluster-randomised before-after study in 4 villages, with 4 villages serving as controls. The primary outcome was the difference in the mean cluster level proportions of mothers directly observed practicing all 5 food hygiene behaviours. At baseline, there were 120 households with a child aged 6-59 months in the 4 intervention clusters, and 119 in the 4 control clusters. The 5 targeted food hygiene behaviours were rare at baseline (composite performance of all 5 behaviours in intervention 1% [standard deviation (SD) = 2%] and in control groups 2% [SD = 2%]). Six weeks after the intervention, the target behaviours were more common in the intervention than in the control group (43% [SD = 14%] versus 2% [SD = 2%], P = 0.02) during follow-up. The intervention appeared to be equally effective in improving all 5 behaviours in all intervention clusters.
Although the question of which elements of the intervention were most effective cannot be determined from this study, the researchers say they suspect that the food preparation setting disruption activity was particularly effective, involving as it did a transformation of the physical environment (repainting, bunting, danglers as behaviour reminder, kitchen tools), the script (mothers committing to behave in a new way), social control (commitment made in front of their neighbours), and the changing designation/purpose of the setting (from kitchen corner to safe food hygiene zone). Figure 2 in the paper shows a typical transformation from all-purpose room used for cooking, eating, sleeping, and keeping animals to a beautiful, bright, and special small kitchen in one corner. Furthermore, the use of emotional motivators such as nurture, disgust, affiliation, and social status may have motivated the key behaviours. The focus on the positive emotional reward of each behaviour (becoming an ideal mother, shiny serving utensils, child's warm tummy, tasty food, social approval) may have helped to reinforce each behaviour, making them part of the daily food preparation routine.
The researchers suspect that performing one behaviour served as a reminder to perform another. For example, mothers practicing cleanliness of serving utensils just before feeding their children were likely to remember to wash their hands just before feeding, as both activities happened simultaneously. Many of the target behaviours happened in sequence; for example, immediately after reheating the food, the mother served the food using serving utensils, then washed her hands, and stored the leftover food properly. It may thus be easier to change multiple behaviours when they are practiced in similar settings and in sequence, when the practice of one can cue another.
The authors reflect: "We attribute the apparent success of the intervention to the use of a systematic process employing global and local knowledge, behavioral theory, and a creative process to design a tailored intervention targeting emotional drivers of food hygiene behavior as well as disrupting food preparation settings....The fact that the intervention was equally effective across targeted behaviors and across clusters and in differing socioeconomic settings suggests that the improvements were due to the effects of the intervention itself. "
They conclude: "The intervention was relatively intense,...and it remains to be seen if the large-scale replication of the package will achieve the same degree of behavior change and whether such changes in behavior can be sustained for the long term."
American Journal of Tropical Medicine and Hygiene, Volume 96, Issue 6, Jun 2017, p. 1415-1426 - sourced from C4D Network Twitter Trawl: 5 – 11 June 2017.
- Log in to post comments