











































Prosocial Polio Vaccination in Israel
Yale School of Public Health (Wells, Fitzpatrick, Pandey, Galvani); The Gertner Institute for Epidemiology and Health Policy Research, Sheba Medical Center (Huppert, Velan); Tel-Aviv University (Huppert); University of Maryland School of Medicine (Fitzpatrick); University of Florida (Singer); University of Waterloo (Bauch)
"Refining the understanding of prosocial vaccination within a population, and accounting for mixed self-interest and prosocial motives, complements past research and allows prosocial behavior to be harnessed further to improve vaccination coverage."
Previous work has shown that prosocial motivation is essential to understand vaccination coverage and that "pure" self-interested behaviour will lead to lower-than-ideal vaccine uptake for disease control. However, determining the degree of prosocial motivation is challenging because the benefits from self-interest and from averting transmission in the community are usually intertwined. The present study examines the circumstances of the vaccination programme against the 2013 silent polio outbreak in Israel, where the social benefits were predominant, as a case study to disentangle the self-interested and prosocial factors associated with vaccination decision making.
In 2013, routine sewage surveillance detected polio, a disease that had been considered effectively eliminated across Israel. To get the outbreak under control, the Israel Ministry of Health proposed a campaign to help stop active community transmission by vaccinating children under 10 years old with the oral polio vaccine (OPV) on top of previously receiving the inactivated polio vaccine (IPV). This presented a unique choice to parents: Children were already protected from paralysis due to IPV, and therefore had no "true" self-interest in vaccinating with OPV.
OPV is a live attenuated vaccine that can lead to vaccine-associated paralytic polio (VAPP) in one per million first doses, whereas IPV does not pose this risk. The risk of VAPP is circumvented by deploying a sequential schedule, initially immunising with 2 IPV doses prior to OPV. This regimen protects recipients from the wild virus as well as VAPP, as was the case for the children targeted by the 2013 campaign. However, the researchers explain that the public did not entirely comprehend the reduced risk of VAPP associated with the Israeli schedule, as people tend to overestimate the likelihood of extremely rare event.
Campaigns around the vaccine aimed to appeal to people's concern for others. This messaging worked: Within the first few weeks of the campaign, 79% of the targeted population sought out and received a single dose of OPV. Over the next 2 years, environmental surveillance showed polio spread declining and a successful containment effort. On April 28 2015, the World Health Organization (WHO) officially declared Israel as a polio-free country.
The researchers examined survey data from 1,015 parents of children under 10 years old, who were surveyed over the phone between January and June 2014 regarding a vaccination campaign that began in August 2013, with a second campaign in early October 2013. The survey captured their reasons for vaccinating their offspring. Parents were classified as aware or unaware of the prosocial nature of the campaign; those who were aware were then classified as prosocial or individualistic (acting only to maximise payoff for their family). The results: 45% were unaware, 17% were individualistic, and 38% were prosocial. People who acted in self-interest (79%) said they hoped to protect their child or family, which is surprising, given that vaccinated children derived no personal benefit from this campaign. Sixteen percent of parents who chose to skip OPV cited vaccine safety as their main reason.
After analysing the data and applying game theory, researchers found that prosocial behaviour was a key driver of OPV vaccination during the 2013 outbreak. In fact, the prosocial model was 17.4 times more likely than the individualistic model to achieve the 79% coverage reported by the Ministry of Health and 17.1 times more likely to achieve the 72% vaccination coverage reported by their survey. Of note, the Arab population - where the outbreak was centralised - had the greatest strength of prosocial behaviour among the 5 Israeli subpopulations. (This result is consistent with previous findings suggesting that prosocial behaviour is often weaker when the benefit goes outside an individual's own social group.)
The researchers found that people who understood the campaign's prosocial nature were likely to have a higher perceived risk of the relative risk of paralysis (vaccine versus infection) compared to those who did not understand the nature of the campaign. This discrepancy in perceived risk is reflected in the survey, which indicates that different information might have been available to each group. Specifically, 78% of the unaware parents vaccinated mainly to protect their child or from a fear of wild-virus polio, while only 59% of aware parents did so for these reasons. These results also highlight that neither group may have been acting with complete knowledge about the campaign, as OPV does not provide their children with any additional protection against paralysis and has no risk of VAPP given previous vaccination with IPV.
According to the researchers, events in Israel following the silent polio outbreak may indicate that social norms about polio vaccination are changing. After the outbreak, the Israel Ministry of Health switched back to a routine vaccination schedule that includes 2 IPV doses followed by an OPV booster. This schedule has been well accepted among the Israeli population, which could indicate a shift to a more prosocial norm. Alternatively, the shift could be attributed to a continuing lack of comprehension regarding the prosocial nature of receiving OPV.
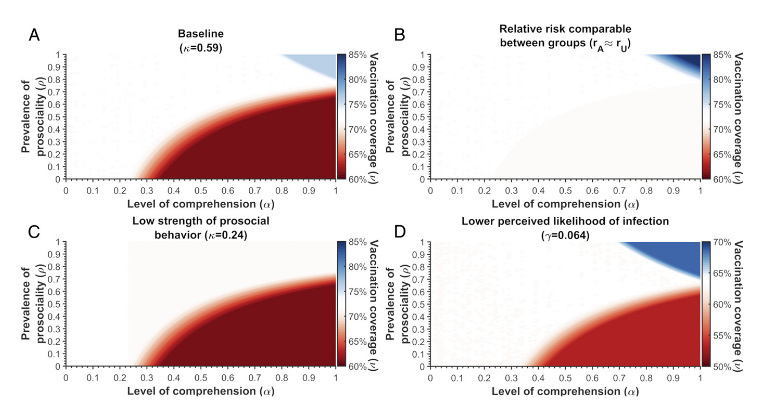
In conclusion, the analysis revealed that the change in vaccination coverage is dependent on whether comprehension of the prosocial nature of the campaign is connected to the perception of vaccine side effects and infection risks, the magnitude of that difference in risk perception between aware and unaware individuals, and how those perceptions change when a previously unaware individual becomes aware. Thus, "education about the vaccine to mitigate the effects of fears and misconceptions surrounding vaccine safety should be the primary focus of communication efforts, with altruistic elements being secondary."
"These results could help guide the design of future OPV campaigns, in the drive toward polio eradication."
Proceedings of the National Academy of Sciences (PNAS) https://doi.org/10.1073/pnas.1922746117 - sourced from "Study on Israel's 'silent' polio outbreak explains why people actually get vaccinated", Inverse, May 25 2020 - accessed on May 27 2020.
- Log in to post comments