











































Social Capital and Utilization of Immunization Service: A Multilevel Analysis in Rural Uttar Pradesh, India
Johns Hopkins Bloomberg School of Public Health (Hasan, Dean, Kennedy, Rao, Gupta); School of Public Policy at Central European University (Ahuja)
"Social capital - especially Social Cohesion of the mothers - appears to be a contextual characteristic of the community, which positively correlates with the utilization of immunization care for children."
Social capital can be defined as the aggregated resources embedded within the social network and relationships of individuals and groups. Literature indicates various pathways through which social capital can influence health-seeking; for example, if immunisation is considered a social norm, a cohesive community will work together to remove barriers to immunisation service. Conducted in the caste-based social structure of rural Uttar Pradesh (UP), India, where social norms, trust, and community support influence health-seeking behaviour, this study examined the association of individual- and community-level social capital on diphtheria-pertussis-tetanus (DPT3) immunisation among 12- to 59-month-old children.
To provide background, the researchers explain that the Expanded Program of Immunization (EPI) was started in India in 1978, followed by the Universal Immunization Program (UIP) in 1985. In 2005, the National Health Mission (NHM) introduced a cadre of frontline workers (FLWs) called Accredited Social Health Activists (ASHAs), as well as the Village Health, Sanitation and Nutrition Committee (VHSNC) and Mission Indradhanush - an intensified immunisation campaign aiming for 90% coverage of full immunisation by 2020. At the community level, the immunisation campaign is led by ASHAs, Anganwadi Workers (AWWs), and Auxiliary Nurse Midwives (ANMs). Every month, the triad of FLWs organises a Village Health Nutrition Day (VHND) to provide routine immunisation to the children in the community. The VHSNC assists FLWs by ensuring community participation, raising awareness, and tracking children who dropped out of the immunisation schedule.
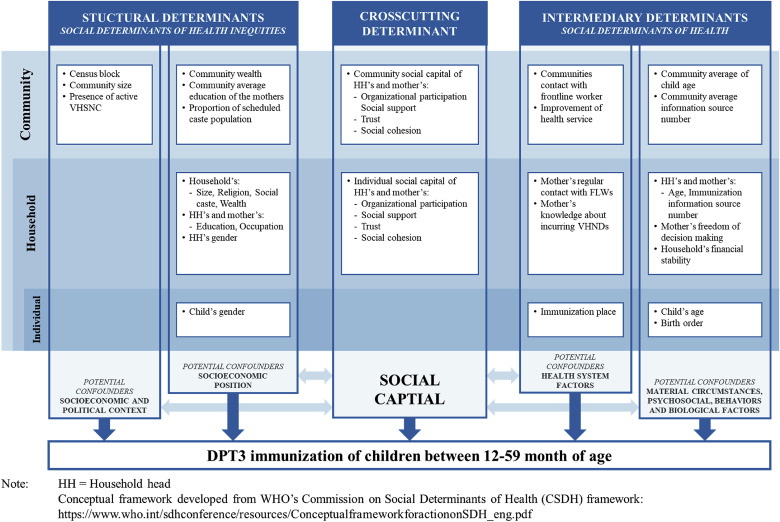
The study uses the World Health Organization's (WHO) Commission on Social Determinants of Health (CSDH) framework to understand social capital's influence on the utilisation of immunisation services. In between structural and intermediary social determinants of health, social capital is situated as the cross-cutting determinant. The constructs of social capital (e.g., trust, cohesiveness, social support, social participation) can independently influence healthcare utilisation and also indirectly influence other structural and intermediary determinants.
The analysis is based on a cross-sectional survey from 2 districts of UP, which included 2,239 children 12-59 months of age (level 1) from 1,749 households (level 2) nested within 346 communities (level 3). The researchers used multilevel confirmatory factor analysis to generate standardised factor scores of social capital constructs (Organizational Participation, Social Support, Trust, and Social Cohesion) of the household heads and mothers both at individual and community level, which were then used in the multilevel logistic regressions to explore the independent and contextual effect of social capital on a child's DPT3 immunisation status.
Multilevel mixed-effect logistic regressions were employed to assess the association of social capital measure with DPT3 immunisation, considering individual children as level 1 (e.g., gender was considered an individual-level structural determinant), households as level 2 (e.g., perceived ability of decision making (How much freedom do you have in making personal decisions) and knowledge about immunisation (the number of sources from where the mother received information about immunisation) were included as intermediary determinants), and Gram Panchayats (GPs) or communities as level 3 (e.g., percentage of mothers in the community with regular contact with FLWs was considered an intermediary determinant).
The results showed that only community-level social cohesion of the mothers was associated with a child's DPT3 immunisation status. Between 2 communities that differ by one standard deviation (SD) of mothers' collective social cohesion, a child living in the community with higher social cohesion of the mothers had 25% higher odds (adjusted odds ratio (AOR) = 1.25, 95% confidence interval (CI) = 1.12-1.54; p = 0.04) compared to a child from a community with lower social cohesion of the mothers. Among other covariates, mother's education and the child's age category presented robust and significant association. In addition, adjusting for all confounders, mother's knowledge of immunisation, community wealth, presence of active VHSNC in the community, and community's contact with FLWs were significantly associated with DPT3 immunisation (p < 0.05).
However, moving from lower to a higher degree of community-level mother's social cohesion, the association between mother's knowledge of immunisation and DPT3 immunissation gradually attenuated and then moved towards negative. The researchers explain that this finding may indicate the influence of informal social control of a highly cohesive community. In other words, the existing social norm and values of a tightly bonded community often discourage its members from adopting behaviours even the members have adequate knowledge to perform that activity.
Another notable finding was that, when the collective social cohesion of mothers was low, higher engagement with FLWs and the community had a positive relationship with DPT3 immunisation of a child. With an increasing level of cohesiveness among mothers, this effect gradually attenuated and led to a null level when the cohesiveness among mothers was highest. It might be the case that FLWs had to proactively engage with those communities where the mothers' social cohesion is low to ensure immunisation of the children. On the other hand, communities with higher social cohesion among mothers were able to organise themselves, ensuring child immunisation irrespective of the level of FLW's interaction with them.
The primary finding of the study was that social capital - specifically, mothers' collective social cohesion - operates mainly at the community level. It was also able to modify - both positively and negatively - the relationship of other social determinants of immunisation. The researchers stress that "There is no cookie-cutter solution to build social capital in any context. So, more in-depth exploration is warranted to understand how social capital is generated within the complex social structure of rural UP." That said, the study "can serve as a starting point to catalyze social capital within the health interventions for achieving wellbeing and the collective development of society."
SSM - Population Health Volume 10, April 2020, 100545. https://doi.org/10.1016/j.ssmph.2020.100545
- Log in to post comments